





22 May, 2020
We wrote in early April to explain the types and functions of therapeutic and vaccines and tests, their pros and cons, attempting to tackle Covid-19. We continue to track global developments on these in real time for your reference here. Six weeks later, we are writing an update on what we have learnt more broadly scientifically in the intervening period and how our understanding is progressing.
This is the first in a three-part blog series:
I. Disease pathogenesis and risk factors
II. Therapeutic and vaccine progress
III. Viral mutation rate emerging strains and serology testing
1. Emerging evidence is indicating Covid-19 is more of a vascular and inflammatory disease than a classical respiratory illness. Intensive Care Unit doctors are reporting that many critically ill patients are in fact not presenting with “classical ARDS” (Acute Respiratory Distress Syndrome) symptoms, and instead demonstrating vascular dysfunction, thrombosis and dysregulated inflammation. Simplistically, this is associated with blood clots within the small vessels in the lungs.
2. Concerningly, cases of a rare multi-system inflammatory disorder have been seen at a 30-fold increased incidence in children – though importantly, these are still extremely low numbers (from 0.3 to 10 per month in the Lancet Bergamo study we reference).
3. It is widely known that the virus infects cells by binding to the ACE2 receptor, but evidence is emerging that risk of severe disease may be in fact linked to lower ACE2 receptor expression (as is the case in males compared to females) due to the implications for vasoconstriction (blood vessel tightening) and inflammation and potentially resulting ARDS.
4. It has been reported that men with prostate cancer being treated with Androgen Deprivation Therapy (“ADT”, e.g. Lupron) are less likely to get severe Covid-19, with the mechanism thought to involve the suppression of the Transmembrane Protease, Serine 2 (“TRMPRSS2”) enzyme, which otherwise is believed to promote engagement of the virus Spike protein with the ACE2 receptor.
5. Emerging studies have indicated that in addition to the well-known risk factors, individuals of blood group A also may be at greater risk than blood group O. We must note these studies are not yet peer reviewed or confirmed, but this phenomenon was also seen in the 2003 SARS epidemic.
Over the last month doctors have been learning more about the clinical progression and presentation of Covid-19. Early evidence is emerging that Covid-19 may not be solely a respiratory disease and have serious vascular complications. New symptoms have emerged over the last month including rare cases of severe inflammatory complications and toxic shock in children [1], loss of sense of smell and taste [2] and rashes appearing on toes [3]. The childhood disease resemble Kawasaki disease, a rare disorder with poorly understood pathogenesis that causes severe vasculitis, often in the coronary artery. In Bergamo, doctors reported a 30-fold rise in the monthly incidence of Kawasaki like disease following the SARS-CoV-2 outbreak [4].
Intensive Care Unit (“ICU”) doctors are reporting that critically ill patients are in fact not presenting with “classical ARDS” symptoms, instead demonstrating vascular dysfunction, thrombosis and dysregulated inflammation [5]. As a reminder, “ARDS” is Acute Respiratory Distress Syndrome: a lung condition where organs have inadequate oxygen supply due to fluid build-up in the lungs. Rather, post-mortem analyses found alveolar damage and clots within the small vessels in the lungs (“microthrombi”) that often present with alveolar haemorrhage [6],[7]. 23% of severe patients have been found to have pulmonary embolisms (a blood clot that blocks a blood vessel in the lung) [8] and post-mortem analyses demonstrated 7/12 patients had undiagnosed deep vein thrombosis (a blood clot in a vein), with pulmonary embolism being the cause of death in 4/12 patients [9].
Overall, it is emerging that SARS-CoV-2 can cause systemic disease with symptoms that are not fully understood. The virus appears to be causing abnormal blood clotting and some element of respiratory failure may be driven by microvascular thrombosis [10].
A largescale study of NHS data has quantified risk factors based on 17 million NHS patient records and 5,683 Covid-19 deaths (Figure 3)[11] and found death from Covid-19 is associated with increased age, obesity, being male (hazard ratio 1.99, 95% CI 1.88-2.10), uncontrolled diabetes (HR 2.36 95% CI 2.18-2.56) severe asthma (HR 1.25 CI 1.08-1.44) and other co-morbidities.
The dual role of ACE 2
The SARS-CoV-2 virus infects cells when the spike protein binds the ACE2 receptor. This binding occurs with remarkably high affinity – 10-20 fold stronger than the SARS-CoV-1 (responsible for the 2003 SARS outbreak) Spike protein which also binds the ACE2 receptor [12].
Possibly counterintuitively despite the virus entering cells via the ACE2 receptor, at risk populations seem to have lower ACE2 receptor expression:
Age results in a decline in ACE2 receptor expression, based on studies in rats [13]
Men have lower ACE2 receptor expression than women. Oestrogen has been shown to increase ACE2 expression and incidentally the gene for ACE2 is found on the X-Chromosome [14]
What is the reason low expression of ACE2 may paradoxically correlate with severe disease?
ACE2 converts Angiotensin II (“Ang II”, a vasoconstrictor, profibrotic and inflammatory molecule) into Angiotensin 1-7 (“Ang 1-7”), a vasodilator (i.e. widening the blood vessels) with anti-inflammatory properties. After infection, the level of ACE2 drops [15], a feature also seen in mice infected with SARS-CoV [16], likely because the virus, along with the ACE2 receptor is internalised and taken up into the host cell (figure 1). This drop in ACE2 results in an increase in Ang II and a decrease in Ang 1-7 (Figure 2). Patients are therefore susceptible to vasoconstriction (narrowing of blood vessels), inflammation and increase in capillary permeability and neutrophil accumulation which may eventually lead to ARDS [17].
High ACE2 receptor expression is likely to increase susceptibility to infection, but the very strong binding affinity of the Spike protein to ACE2 means even those with low ACE2 expression can still get the disease. However, those with low ACE2 expression are at risk of a critical drop in Ang 1-7 and severe vascular effects [18]. A study that infected mice with the SARS-CoV spike protein showed that this was sufficient to decrease ACE2 expression and drive lung injury, but could be mitigated by Losartan, an approved blood pressure drug which is an Ang II receptor antagonist (i.e. it competes with Ang II by binding to and blocking the receptor which Ang II normally binds to, preventing its normal function [19]). Consistently and reassuringly, ACE-Inhibitors (note – not ACE2) which inhibit the formation of Ang II, and were initially a cause of concern due to upregulation of ACE2, have actually been shown to not to increase the mortality rate. A pre-print from King’s College London reported that of patients exposed to ACE Inhibitors 14% (5/37) required intensive care compared to 29% (48/168) patients who had not been exposed to ACE inhibitors [20],[21]. There is clearly a trade-off to be had with drugs that may both increase the susceptibility to cells being infected, but also reduce the severity of injury caused by the disease, and more data is needed.
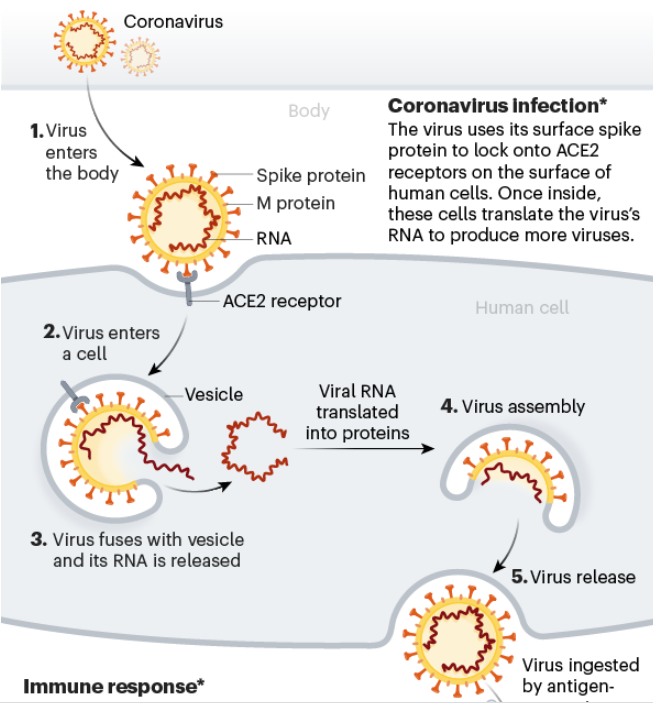
Figure 1: Viral binding to ACE2 receptor results in internalisation and loss of ACE2 receptor from the cell surface. Source: Nature [22].
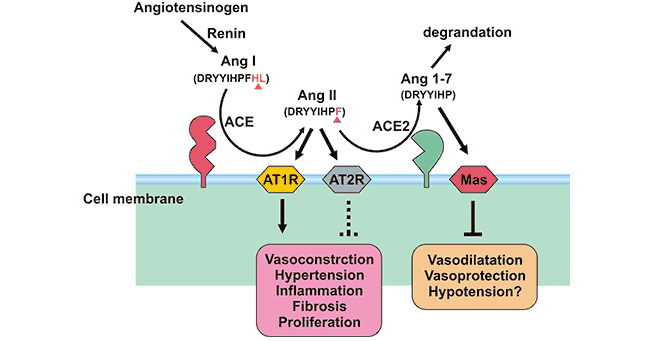
Figure 2: Angiotensinogen pathway showing ACE2 receptor converts Ang II to Ang 1-7. Ang 1-7 binds to the MAS receptor trigger vasodilation and anti-inflammatory signals. Source: https://www.cusabio.com/c-20982.html
Risk factors beyond ACE 2
We do not fully understand why young children are at low risk of the virus (notwithstanding the rare, but severe cases of Kawasaki like disease). Widespread community testing in Korea showed children under 10 accounted for less than 1% of laboratory confirmed cases [23] and a similar low incidence was seen in Iceland [24]. This is contrary to the pattern seen in influenza when young children are often at risk, but comparable to the 2003 SARS outbreak. Potential explanations include reduced co-morbidities, reduced lung inflammation from pollutants, or a dominant T cell response from the immune system which is effective at clearing the virus.
Beyond ACE2 levels, men may be at higher risk due to lifestyle choices (e.g. alcohol consumption) and obesity resulting in higher co-morbidities. Theories are emerging that oestrogen may have a protective effect on women, which is being further investigated [25]. Recently, it has been reported that men with prostate cancer being treated with Androgen Deprivation Therapy (“ADT”, e.g. Lupron) were less likely to get severe Covid-19, with the mechanism thought to involve the suppression of the Transmembrane Protease, Serine 2 (“TRMPRSS2”) enzyme [26]. Finally, increased male risk may not be specific to SARS-CoV-2 – it has been reported that at times of famine and epidemics women seem to survive better [27].
Diabetes, especially unregulated diabetes, is associated with increased risk of disease severity and mortality (Figure 3). Proposed mechanisms include a reduced innate immune response in diabetic patients or an association with an exaggerated cytokine response which may contribute to more severe inflammation and ARDS. Interestingly, ACE2 function is reduced in diabetic patients, perhaps due to increased glycosylation, which as discussed above may increase the severity of the disease through signalling increased vasoconstriction, inflammation and fibrosis.
Curiously two studies have indicated individuals of blood group A are higher risk of severe Covid-19 infection than blood group O. Blood group A individuals express the “A” antigen on red blood cells, whereas blood group O individuals do not [28],[29]. A similar finding was also reported for SARS-CoV-1, the virus behind the 2003 SARS outbreak [30]. The mechanism for this is not clearly understood.
It does also appear to be the case that those from non-white ethnicity are also at greater risk of severe disease. Again, it is poorly understood whether this is related to genetic or environmental factors.

Figure 3: Hazard Ratio (logarithmic scale) for potential risk factors based on NHS England Dataset involving 5,683 deaths. Source: OpenSAFELY collaborative, pre-print May 2020.
The second part of this three-part blog series will be coming shortly. Watch this space!
[1] https://discoveries.childrenshospital.org/covid-19-inflammatory-syndrome-children/, https://www.theguardian.com/world/2020/may/09/children-coronavirus-death-kawasaki
[2] https://www.ncbi.nlm.nih.gov/pubmed/32215618?dopt=Abstract
[3] https://www.bbc.co.uk/news/health-52493574
[4] https://www.thelancet.com/action/showPdf?pii=S0140-6736(20)31103-X
[5] https://www.esicm.org/wp-content/uploads/2020/04/902_author_proof.pdf
[6] https://www.medrxiv.org/content/10.1101/2020.04.06.20050575v1.full.pdf
[7] https://onlinelibrary.wiley.com/doi/abs/10.1111/his.14134
[8] https://pubs.rsna.org/doi/10.1148/radiol.2020201544
[9] https://www.cidrap.umn.edu/news-perspective/2020/05/autopsies-covid-19-patients-reveal-clotting-concerns
[10] https://www.sciencedaily.com/releases/2020/04/200423143100.htm
[11] https://www.medrxiv.org/content/10.1101/2020.05.06.20092999v1
[12] https://www.frontiersin.org/articles/10.3389/fped.2020.00206/full
[13] https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7094566/
[14] https://www.ncbi.nlm.nih.gov/pubmed/28661206
[15] https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7167588/
[16] https://www.nature.com/articles/nm1267
[17] https://www.ahajournals.org/doi/10.1161/JAHA.120.016219
[18] https://jamanetwork.com/journals/jamacardiology/fullarticle/2764300#hvp200010r4
[19] https://www.nature.com/articles/nm1267
[20] https://www.univadis.co.uk/viewarticle/aceis-arbs-linked-to-reduced-mortality-in-covid-19-718573
[21] https://www.medrxiv.org/content/10.1101/2020.04.07.20056788v1.full.pdf
[22] https://www.nature.com/articles/d41586-020-01221-y
[23] https://europepmc.org/article/PPR/PPR117801
[24] https://www.nejm.org/doi/10.1056/NEJMoa2006100
[25] https://covid.joinzoe.com/post/oestrogen-covid
[26] https://www.pcf.org/blog/breaking-news-adt-may-offer-some-protection-from-covid-19-in-men-with-prostate-cancer/
[27] https://www.pnas.org/content/115/4/E832
[28] https://www.medrxiv.org/content/10.1101/2020.03.11.20031096v2
[29] https://www.medrxiv.org/content/10.1101/2020.04.08.20058073v1
[30] https://jamanetwork.com/journals/jama/article-abstract/200582
DISCLAIMER
This document and the information contained herein is for information purposes only. The document is provided on a non-reliance basis contains forward looking statements and opinions of the manager, which may be subject to change or revision without notice. Some information contained herein was based on, obtained or derived from data published or prepared by other parties (“Third-Party Information”).
None of Ahren or its affiliates, directors, officers, employees, partners, shareholders or agents (each, an “Ahren Party”) assumes any responsibility for the accuracy of the document or any Third-Party Information. No Ahren Party makes any representation or warranty, express or implied, as to the accuracy or completeness of this document or any Third-Party Information and no Ahren Party shall have any liability to the recipient or any other person relating to or resulting from the use of or reliance on any such information contained herein or any errors therein or omissions therefrom. No warranty, express or implied, or assurance is given by the manager or any of its directors, officers, members or employees.
Nothing contained in this document may be relied upon as a guarantee, promise, assurance or a representation as to the future. Except as otherwise indicated, the information provided in this Investor Letter is based on matters as they exist as of the date listed on the cover and not as of any future date, and will not be updated or otherwise revised to reflect information that subsequently becomes available or circumstances existing or changes occurring after the date hereof. The views expressed in this Investor Letter are subject to change based on market and other conditions. In considering the performance information contained herein, prospective investors should bear in mind that past, forecasted or targeted performance is not necessarily indicative of future results, and there can be no assurance that comparable results will be achieved.
Neither Ahren nor any of its affiliates makes any representation or warranty, express or implied, as to the accuracy or completeness of the information contained herein, and nothing contained herein should be relied upon as a promise or representation as to past or future performance of Ahren or the fund or any other entity.
The recipient acknowledges that, to the maximum extent permitted by law, each of Ahren and its related parties or affiliates disclaims all liability to the recipient or to any other person for any expense, cost, loss or damage of any kind including direct, indirect or consequential loss or damage (however caused, including by negligence) incurred by any person arising from or relating to any information included or omitted from this Investor Letter, whether by reason of such information being inaccurate or incomplete or for any other reason. This Investor Letter does not constitute and should not be considered as any form of financial opinion or recommendation. The recipient should conduct its own inquiries as to the adequacy, accuracy, completeness and reliability of any information, whether such information is contained in this Investor Letter or not, relating to Ahren or the fund.
No action should be taken by any recipient which, in the light of the information herein, would render such action illegal or violate any applicable laws or regulations. Neither the manager nor any of its directors, officers, members or employees accepts any liability whatsoever for its accuracy or any action taken by a recipient which is illegal or in violation of any applicable law or regulation as a result of receiving this document and its contents.
The Site cannot and does not contain medical or health related advice. The medical or health information is provided for general informational and educational purposes only and is not a substitute for professional advice. Accordingly, before taking any actions based upon such information, we encourage you to consult with the appropriate professionals. We do not provide any kind of medical or health advice.
The Site does not offer, and should not be construed in any way as offering legal, regulatory or tax advice. The information is provided for general informational purposes only and is not a substitute for professional legal or tax advice.
THE USE OR RELIANCE OF ANY INFORMATION CONTAINED ON THIS SITE IS SOLELY AT YOUR OWN RISK.
 22 December, 2020
Professor Zoubin Ghahramani: Ahren Podcast Series – A Glimpse into the Future with Ahren’s Science Partners
22 December, 2020
Professor Zoubin Ghahramani: Ahren Podcast Series – A Glimpse into the Future with Ahren’s Science Partners
 18 December, 2020
Ahren Innovation Capital’s Annual Symposium – Science Partner Panel Highlights 2019
18 December, 2020
Ahren Innovation Capital’s Annual Symposium – Science Partner Panel Highlights 2019




